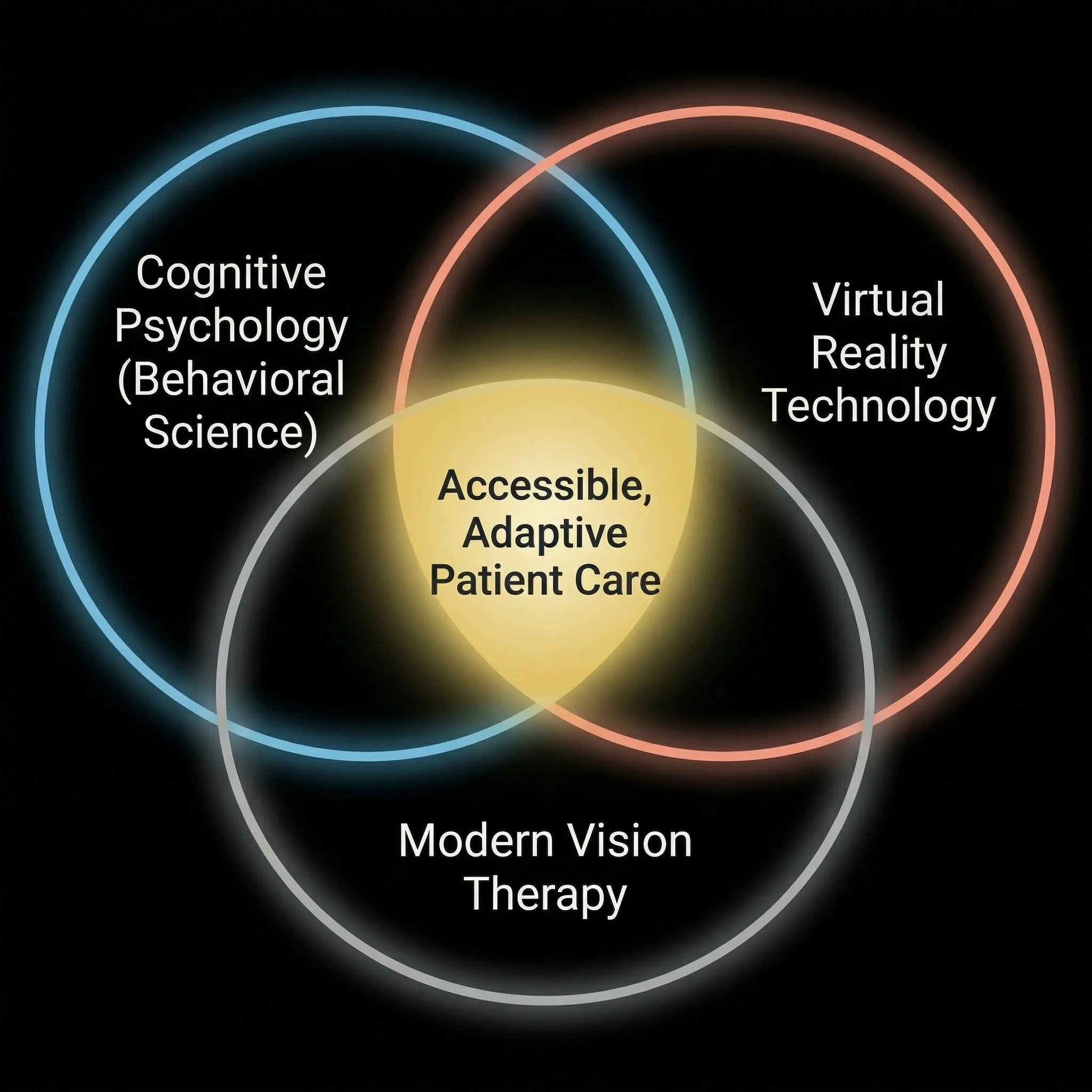
Case Study and Feasibility Assessment
Democratizing Vision:
Virtual Reality for Binocular Dysfunction
by Steven Berg, Ph.D.
February 2026
GOAL: An assessment of the feasibility, viability, and benefits of transitioning orthoptic treatment from clinical standard-of-care to dynamically-adjusted, home-based VR environments

CONCLUSION: Using VR technology for orthoptic treatment (to help some of the ~3-5% of those in the global population with stereoblindness) has the potential to transform vision therapy into a scalable, accessible, and life-changing digital intervention
TAKEAWAY: By reducing the environmental friction of traditional care and replacing the manual burden on researchers with automated eye-tracking calibration features, these technologies have the potential to solve the problem of a high-value unmet need
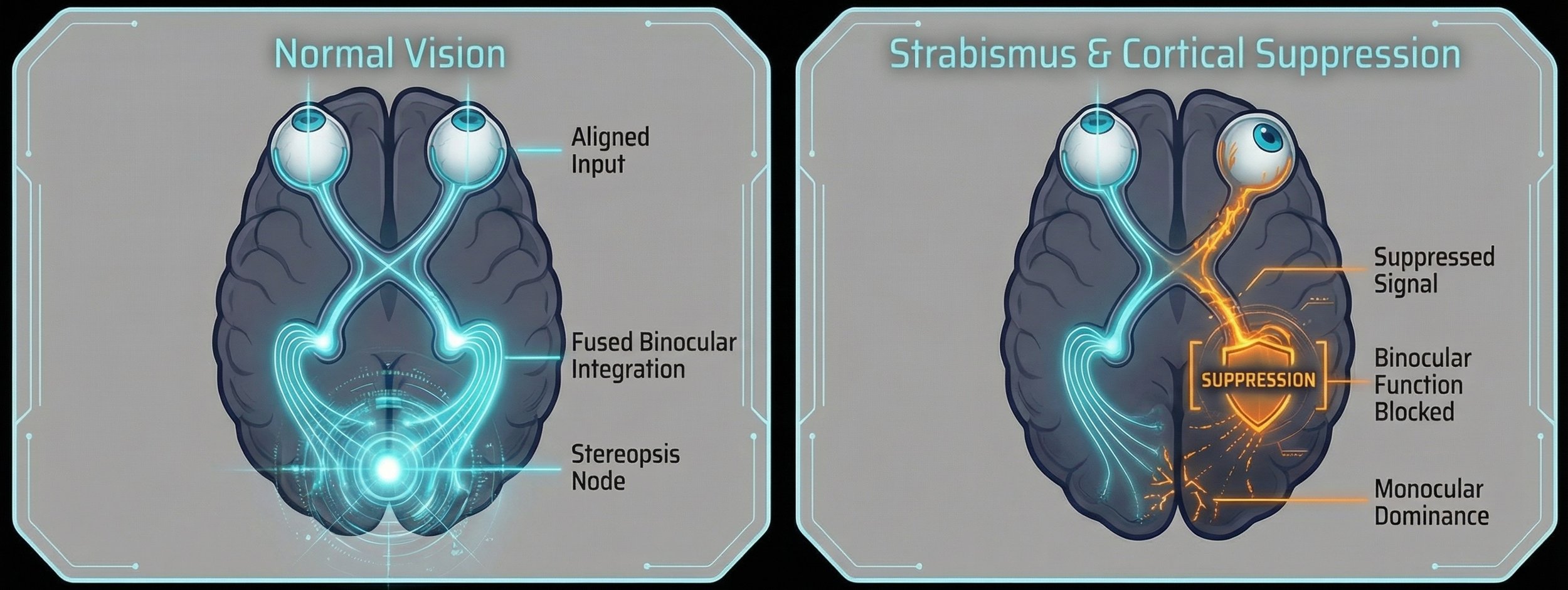
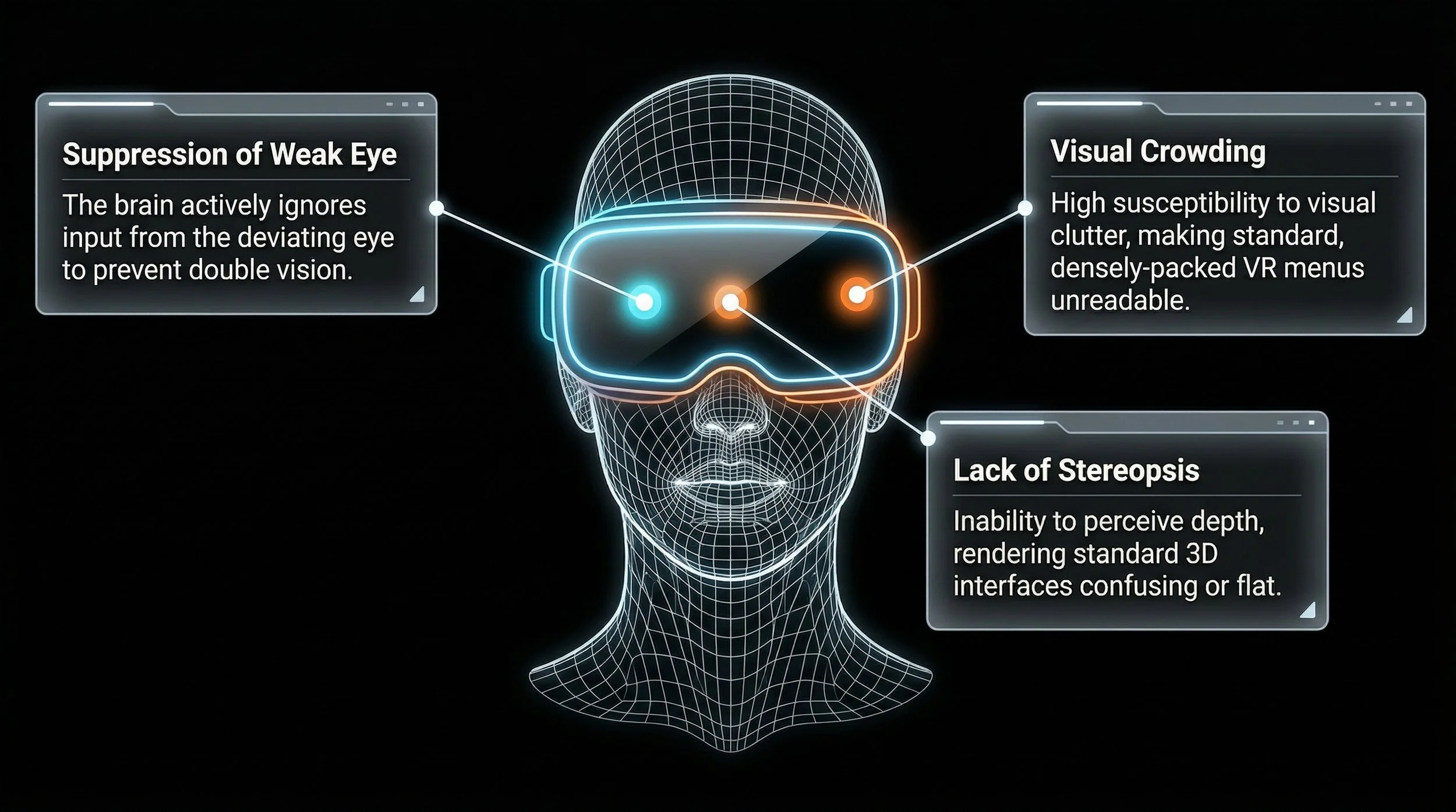
The Neurological Roadblock: Misalignment and Cortical Suppression
When human eyes misalign (strabismus), the visual system received highly disparate images, causing diplopia (double vision)
To compensate, the brain actively suppresses vision in the deviating eye.
The neural hardware for depth perception exists, but active suppression prevents disparity-selective neurons from fusing binocular information
Empathizing with the User
Living with binocular dysfunction (such as strabismus or amblyopia) inherently introduces friction into a user's daily life. When the visual system suppresses vision in one eye to avoid diplopia, it impacts depth perception and quality of life
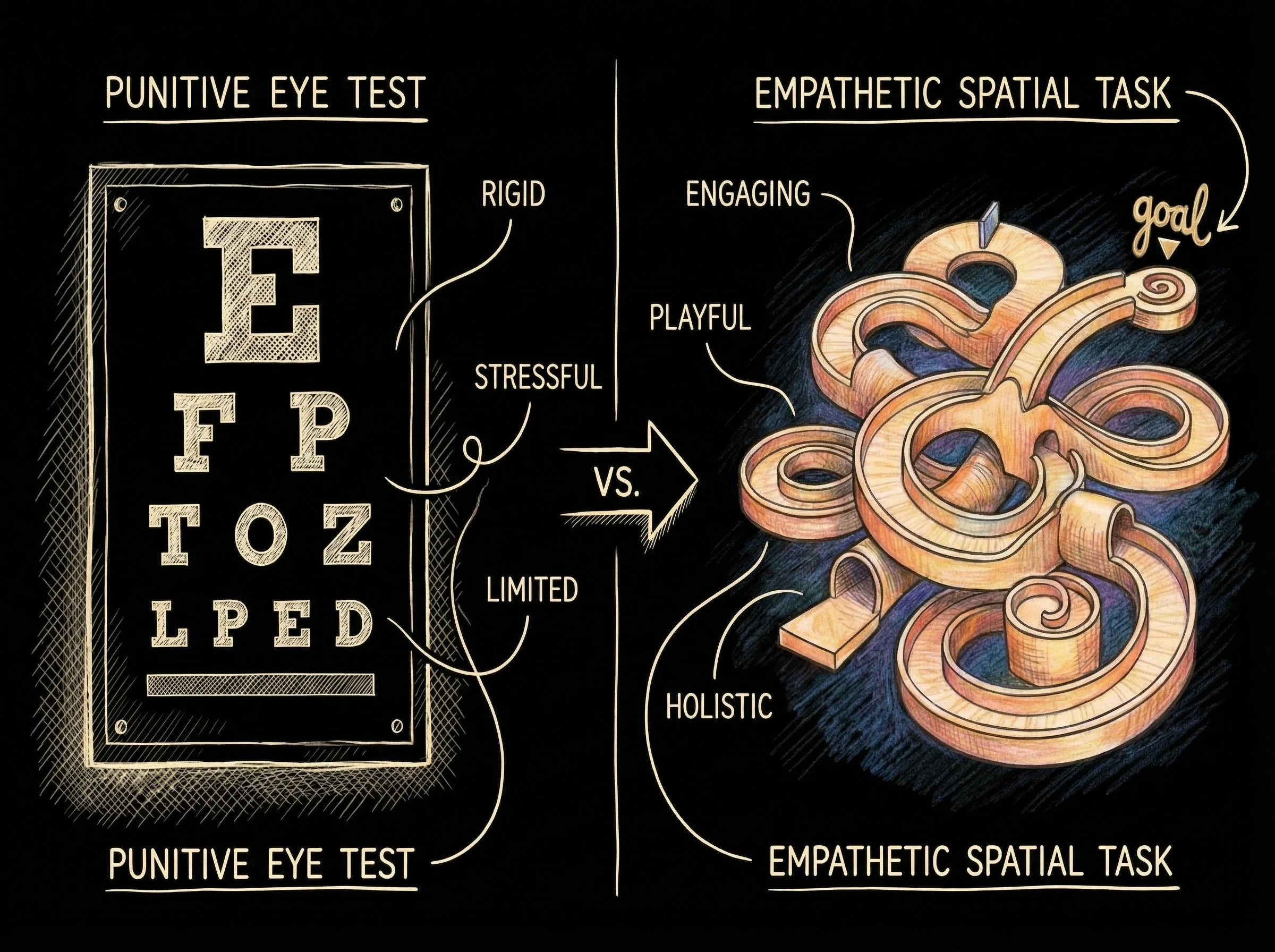
Current Standard of Care (SoC) therapies often exacerbate this friction rather than relieve it; to design a truly viable solution, we must first deeply understand the pain points of the current user journey

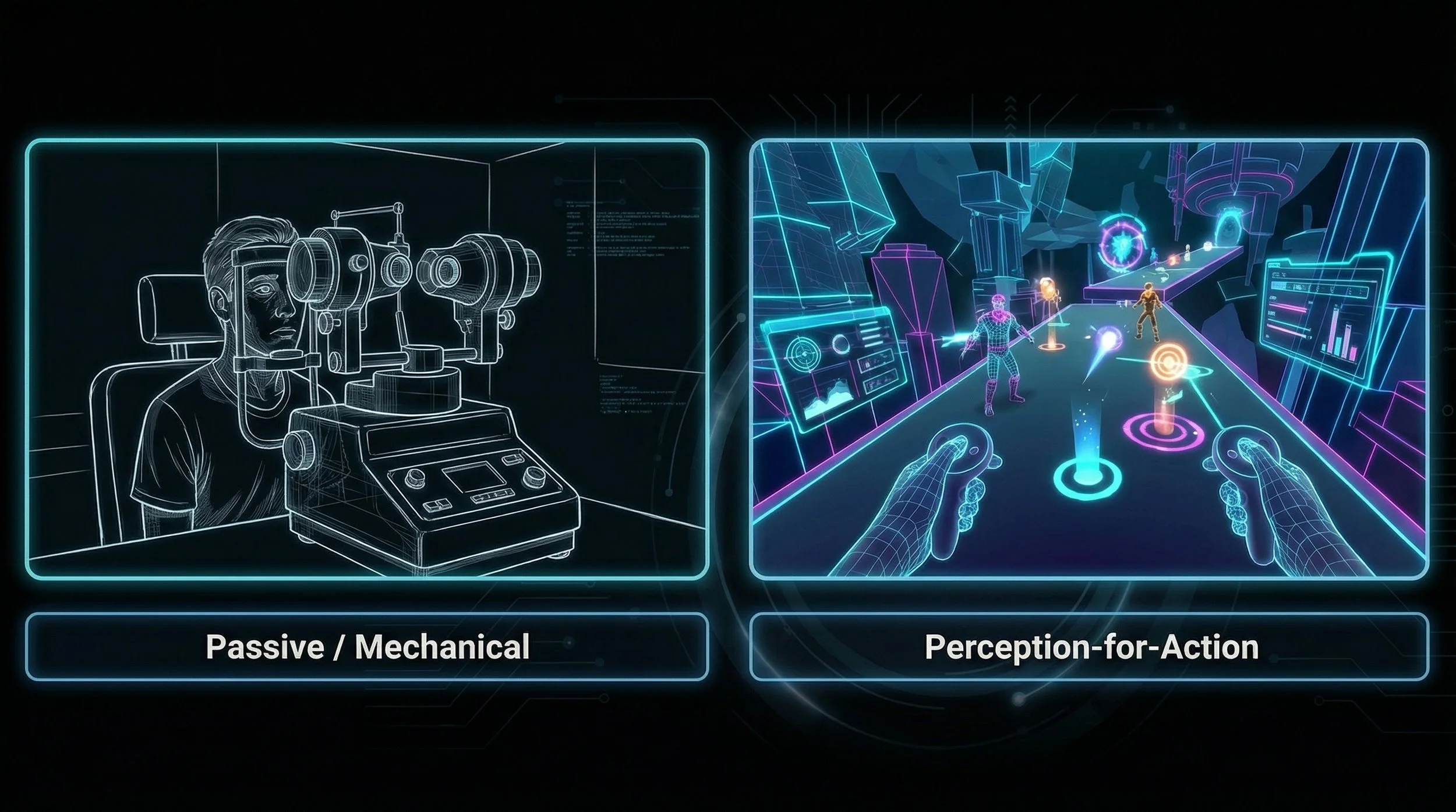
Standard-of-Care vs. VR Intervention
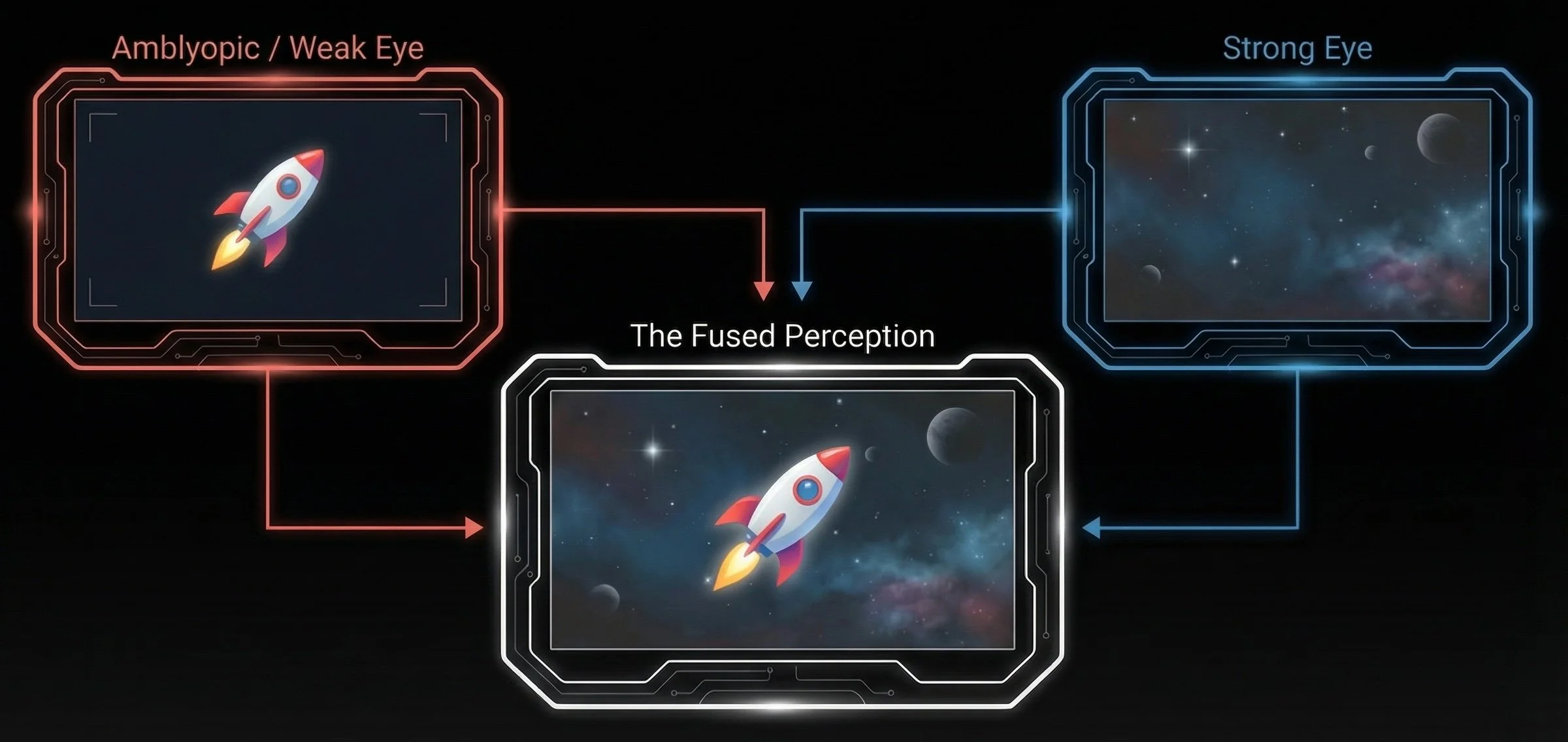
By shifting from physical, clinic-based treatments to a head-mounted display (HMD) ecosystem, we radically alter the user experience dimensions

By reducing contrast in the strong eye and placing critical objectives in the weak eye, the software achieves what a physical eye patch attempts, but does so while preserving and actively training binocular fusion
The Hebbian Principle: Neurons that fire together, wire together!
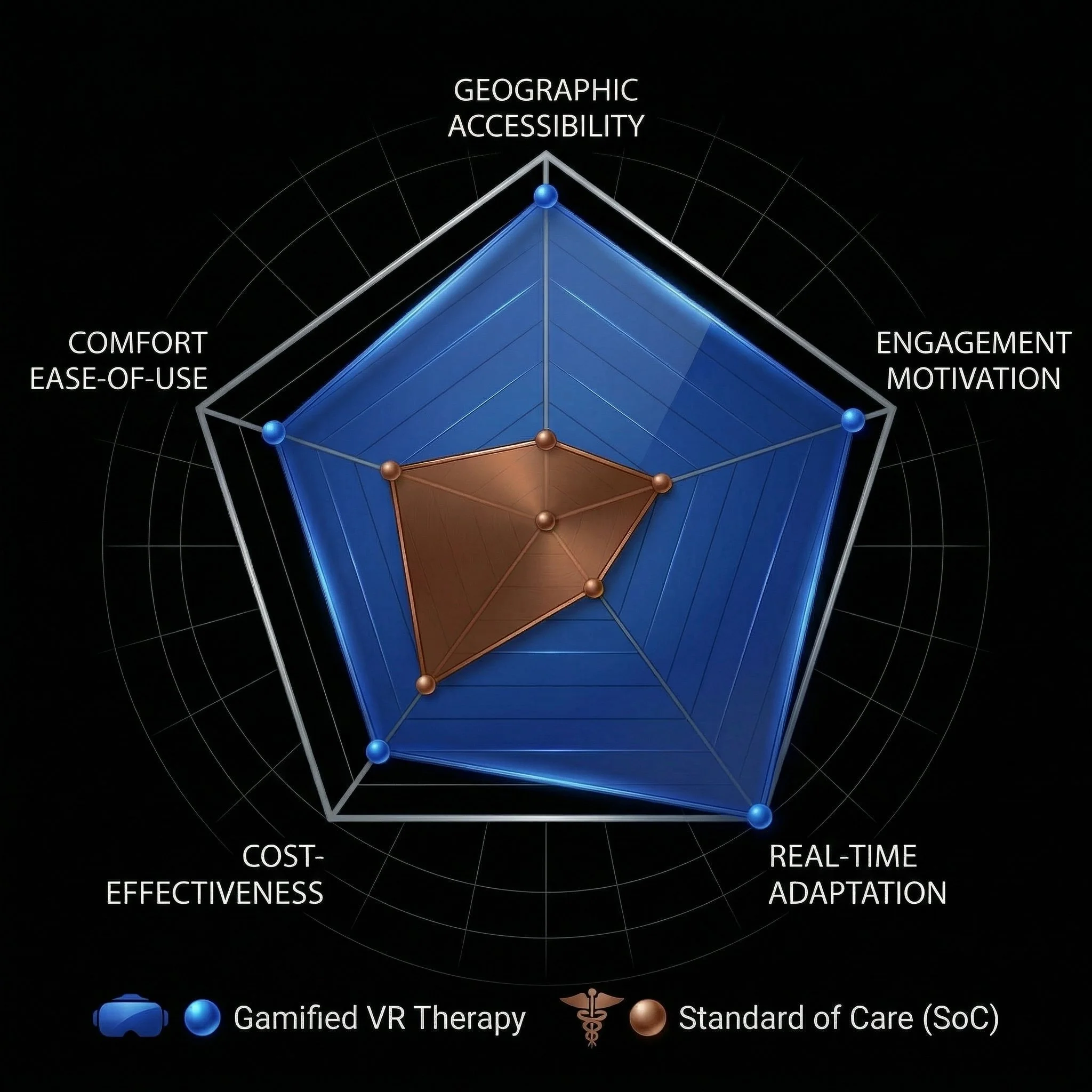
The radar chart (below) visualizes the stark contrast in user metrics between traditional clinical visits and an adaptive, gamified VR therapy approach
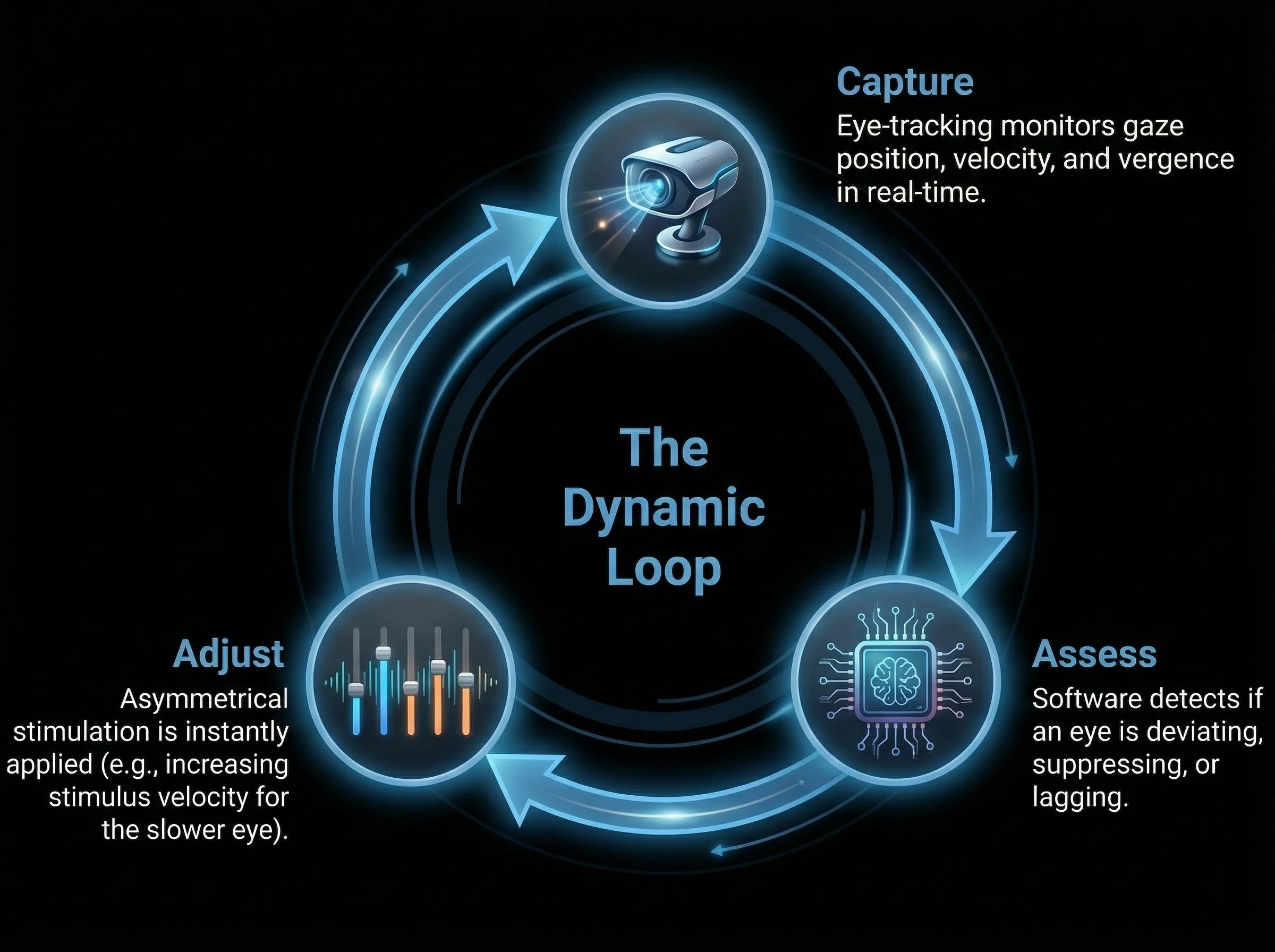
Real-time adaptation: Gaze-contingent displays adjust instantly to the user’s eye movements, removing the friction of manual calibration
Replacing clinical tools with gamified environments (e.g., squashing virtual bugs) transforms a chore into an immersive experience
Designing the Frictionless Journey
The viability of scaling this technology relies on minimizing the cognitive and physical load on the patient
The system adapts to the user, not the other way around
Real-time tracking eliminates the friction of manual clinical adjustments
The patient stays fully immersed while the software does the heavy lifting
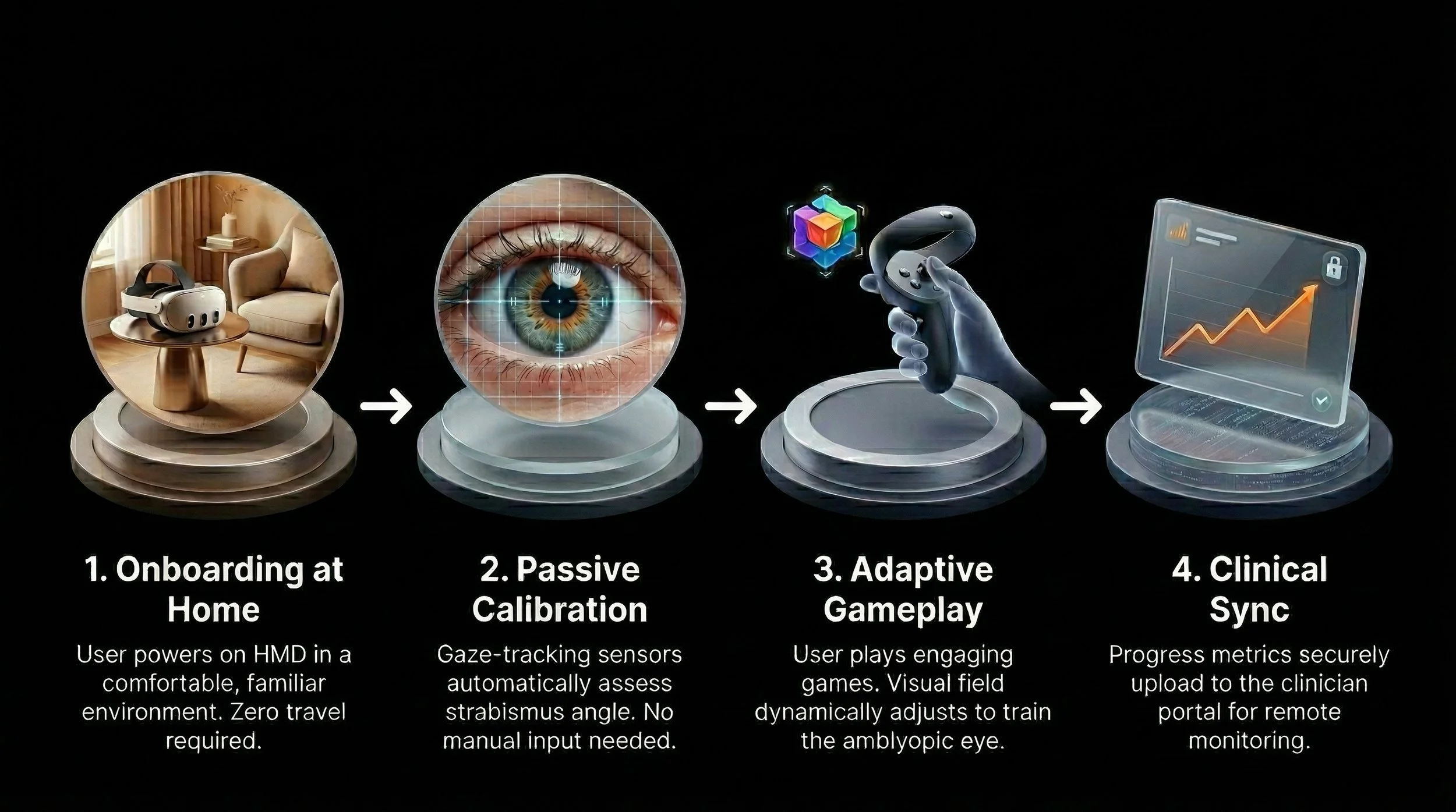
The proposed VR ecosystem introduces a streamlined, home-based process flow that prioritizes user autonomy and continuous, passive data collection for clinicians
Feasibility & Viability Outcomes
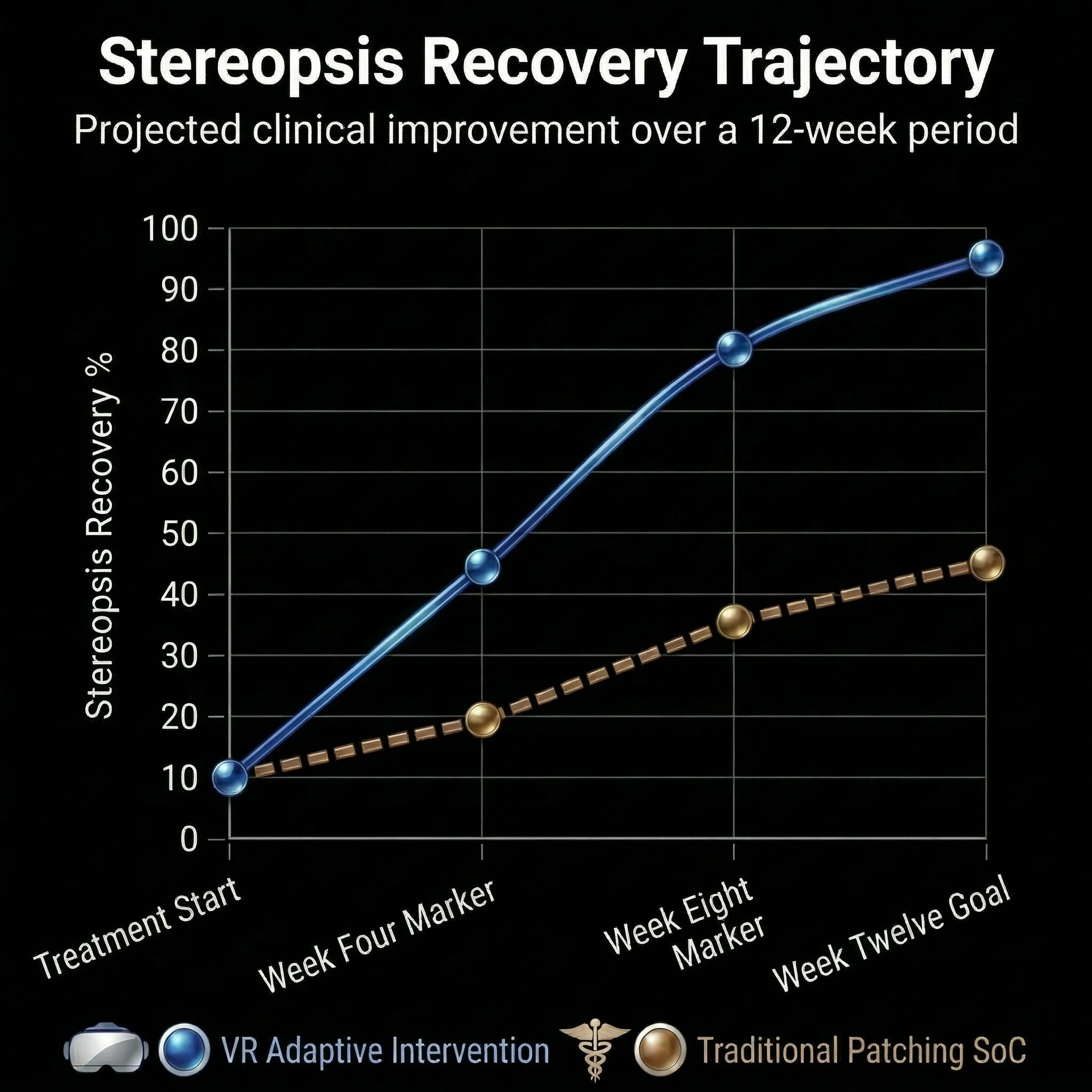
By addressing core user needs, the implementation of VR technology has the potential to yield profound quantitative improvements in both adherence rates and clinical timelines
Designing for the user has the potential to directly translate to measurable clinical success
Repetition is required for cortical plasticity, but repetition causes boredom
VR integrates multi sensory feedback (visual, auditory, & proprioceptive) within an interactive game loop; this transforms a tedious medical chore into intrinsically-motivated gameplay, driving top-down executive learning
What looks like a measure of success?
Decreased drop-out rate among low-compliance users as compared to standard-of-care
Increased proportion of stereopsis recovery among VR therapy patients relative to traditional treatments
Actionable Insights and Deliverables
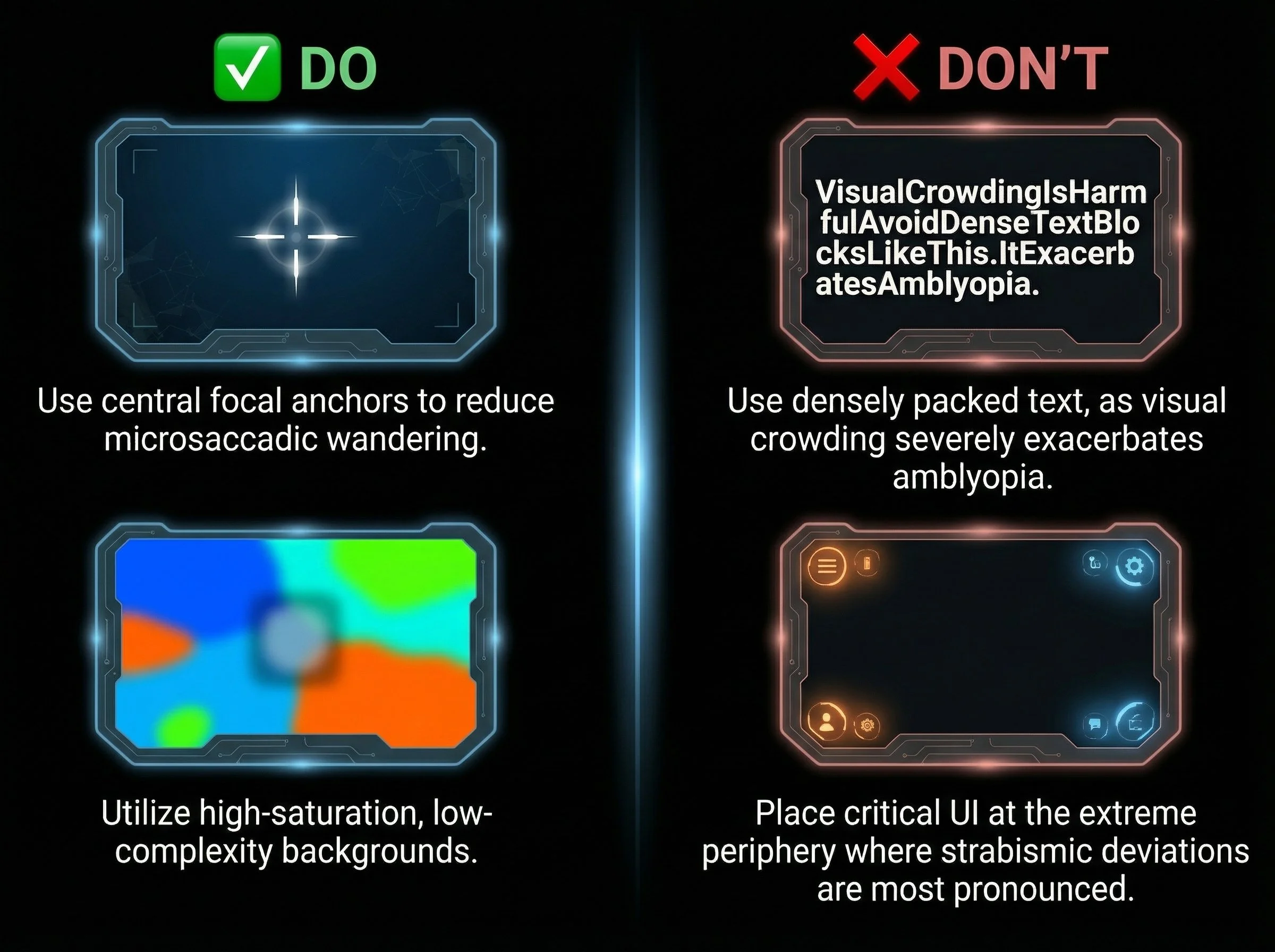
UI Contrast & Typography
Insights:
Users have inherent visual deficits (e.g., amblyopia, diplopia)
Smart spatial layout actively limits visual suppression and keeps the user’s fovea engaged exactly where therapeutic value is highest
Deliverables:
Implement dynamic UI scaling
Base fonts must exceed standard accessibility minimums
Avoid low-contrast overlays
Ensure crucial navigational elements rely on shape and position, not just color or fine detail
Fatigue Mitigation
Insight: VR can induce cybersickness, nausea, and/or queasiness; orthoptic training induces eye strain
Deliverables:
Design 10-15-minute modular gameplay loops
Implement mandatory “cool-down” visual environments (e.g., gazing at a distant, static horizon) to rest ocular muscles between intense therapeutic sequences
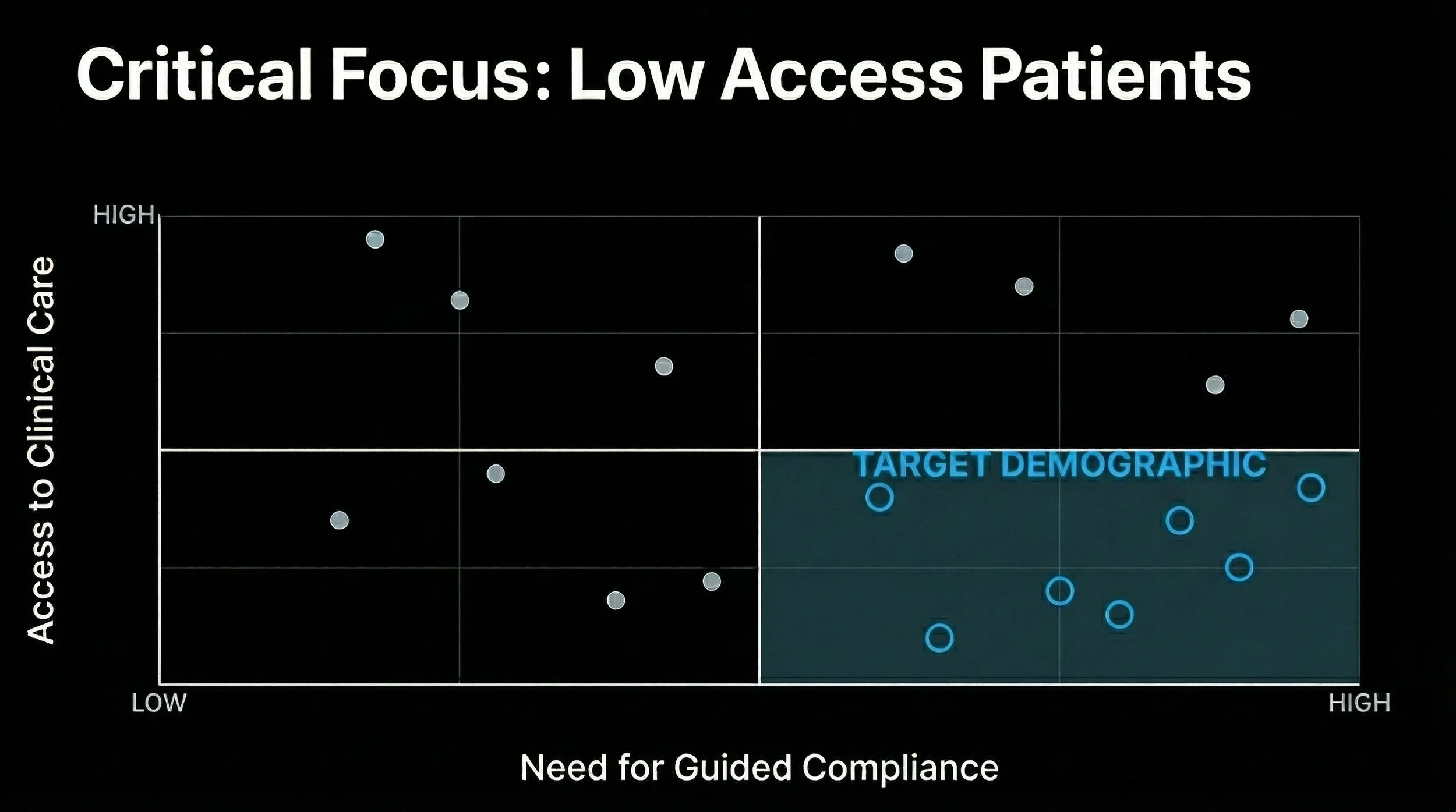
Guided Compliance and Access
Insight: Users may feel anxious about their condition and/or new technology
Deliverables:
A guided, voice-narrated tutorial environment that praises micro-achievements
The system must never frame a failed visual task as a “loss,” but rather as data used “to help the system adjust to you”
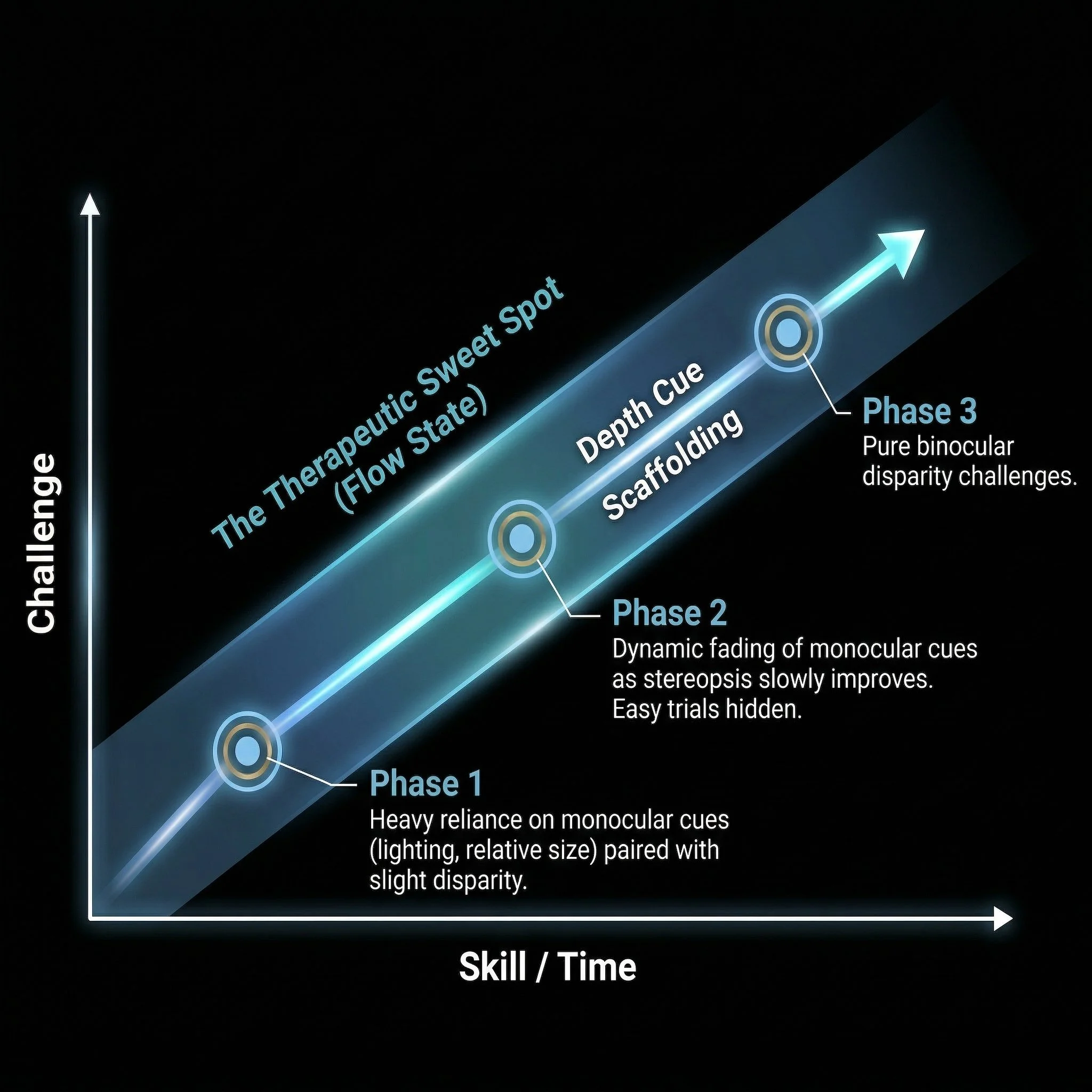
Empathetic Onboarding
Insights:
The first 5 minutes dictate long-term compliance; gradual immersion actively prevents immediate binocular stress, gently introducing the virtual environment before therapeutic demands begin
If therapy is too hard, the brain suppresses the weak eye; if too easy, neuroplasticity stalls
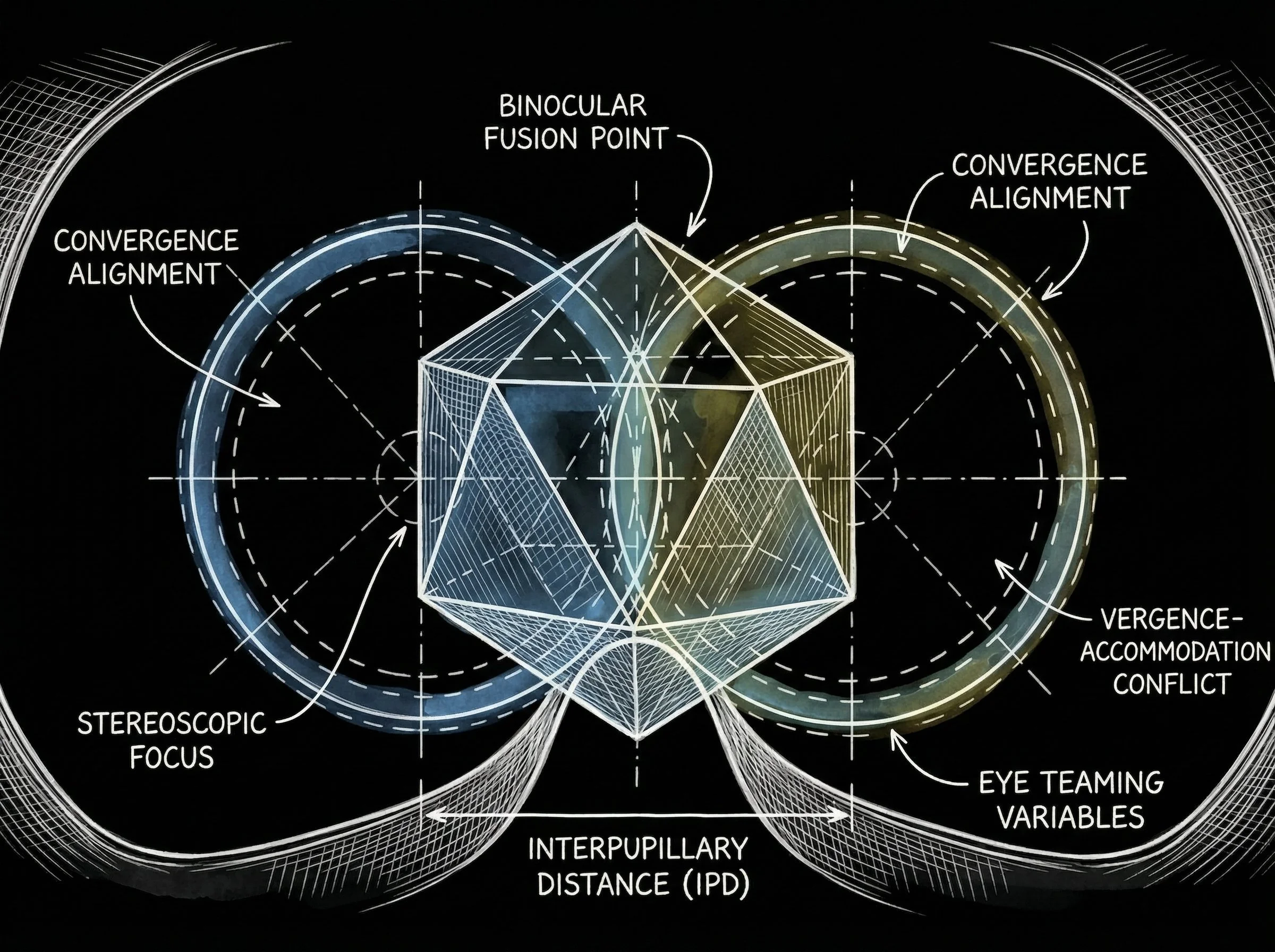
Deliverables:
Physical interpupillary distance (IPD) calibration to prevent motion sickness
Establishing visual acuity using large, high-contrast targets without visual crowding
Slowly fading in peripheral cues before introducing central disparity challenges
Dynamic scaffolding keeps the patient perfectly balanced to prevent cognitive overload and visual fatigue
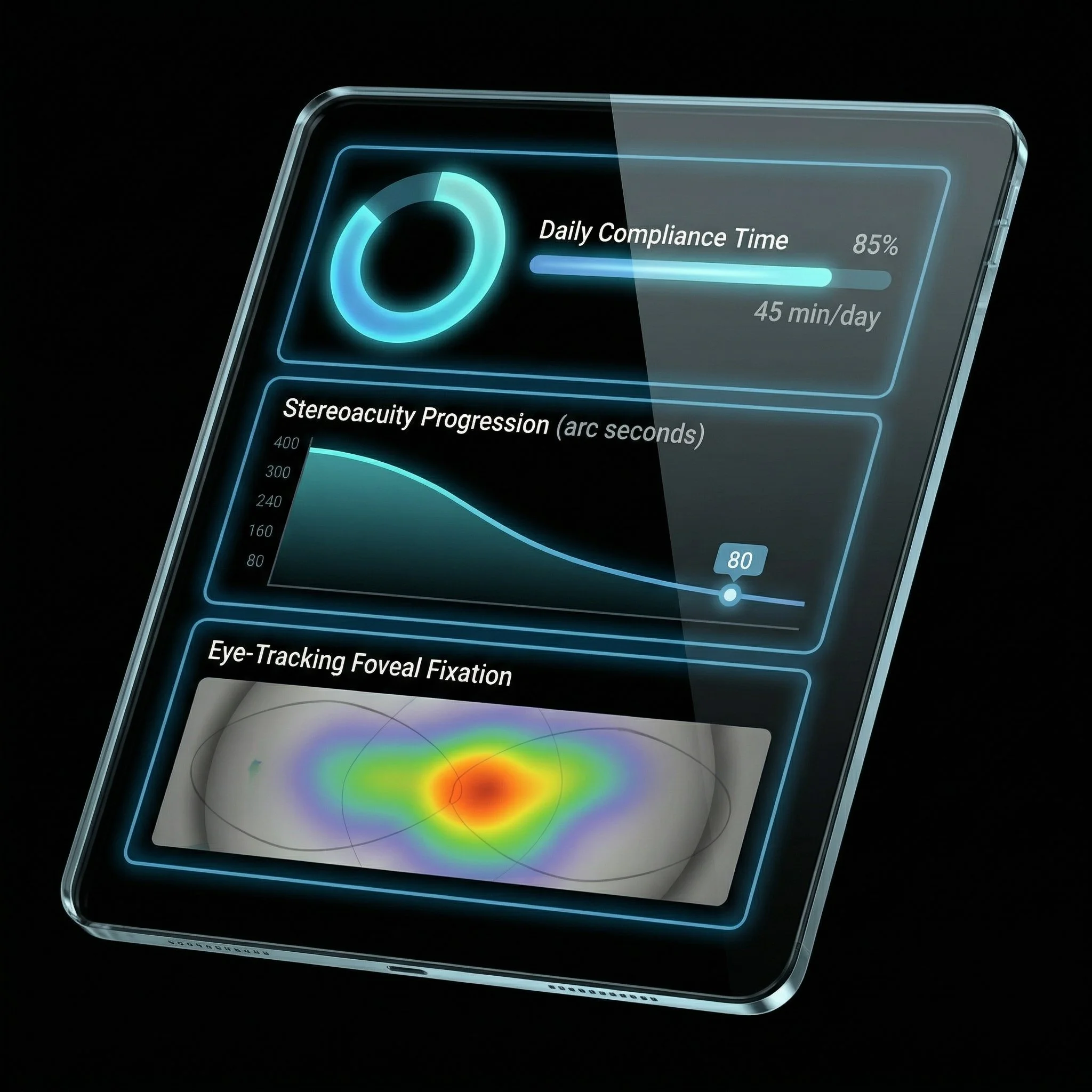
Clinician Dashboard
Insights:
The secondary user is the clinician who needs easily accessible and equally easily interpretable data
Home-based VR does not remove the clinician; it elevates them from taskmaster to data analyst
Deliverables:
A web-based portal translating raw gaze-tracking coordinates into simple, actionable visual heatmaps and compliance trend lines
Enable quick, data-driven remote adjustments
Orthoptists can remotely monitor compliance, adjust baseline parameters, and provide highly informed telemedicine oversight

Efficacy, Outcomes, & Realities
Expected benefits:
Improved patient compliance via intrinsic gamification
Quantifiable reduction in cortical visual suppresion
Improved stereo acuity and reliable depth perception
Current limitations:
Hardware weight and IPD minimums restrict use for children under 7 years
Requires a baseline of binocular potential
Not a standalone cure for large-angle constant strabismus requiring surgical intervention
Although VR is a powerful tool for anti-suppression and perceptual learning, it must be used to enhance — rather than replace — thorough clinical oversight; practitioners must continue to prioritize careful patient selection